
A rare disease is defined as a condition that affects fewer than 200,000 people in the United States. Trisomy 18, also known as Edwards syndrome, is a rare genetic condition that falls within this category. It occurs when an extra copy of chromosome 18 is present in some or all of the body’s cells. This additional genetic material can disrupt typical development, often resulting in significant medical and developmental challenges. Trisomy 18 affects approximately 1 in 5,000-6,000 live births.
Trisomy 18 Common Characteristics and Complications
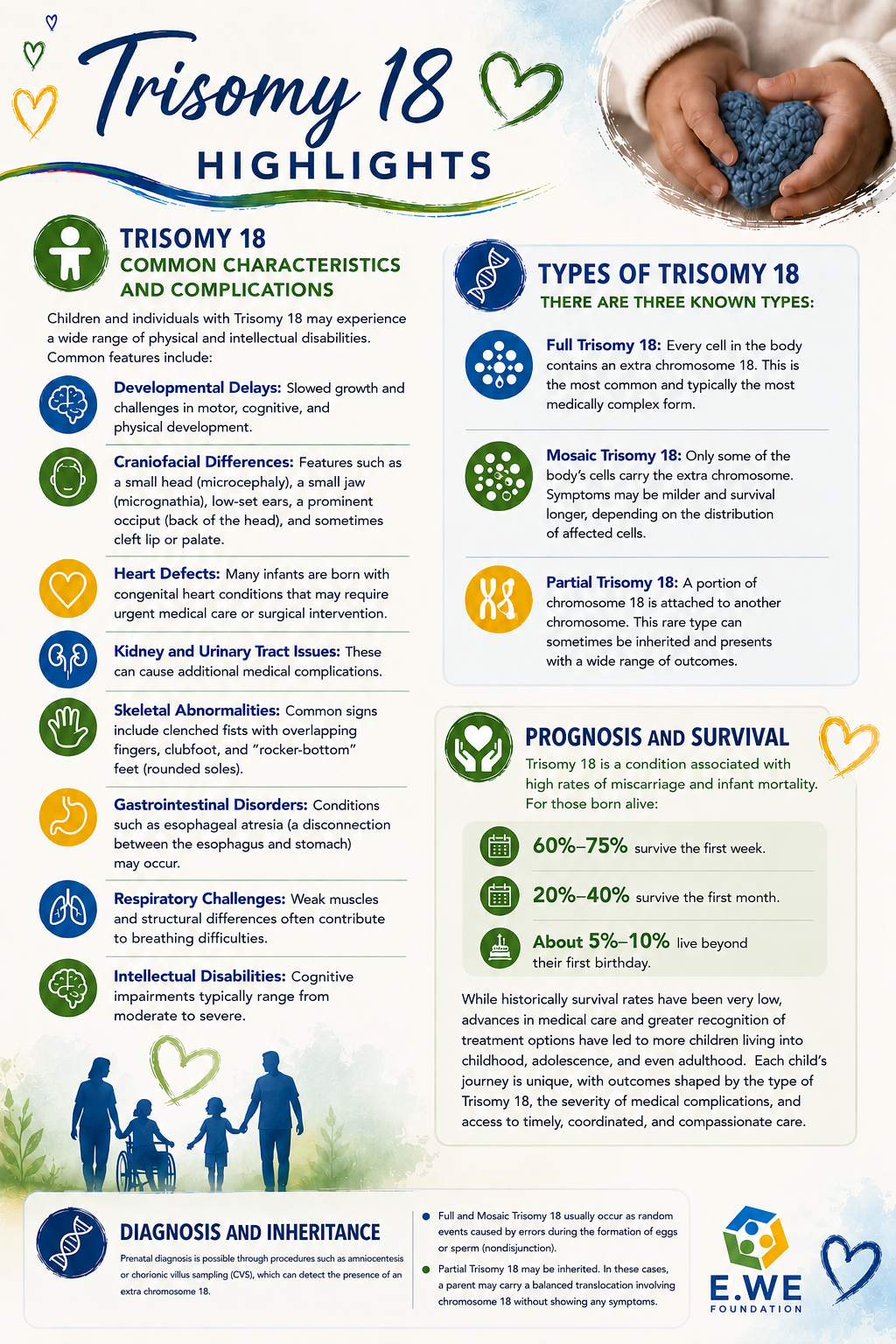
Infants born with Trisomy 18 may experience a wide range of physical and intellectual disabilities. Common features include:
- developmental delays
- craniofacial differences
- heart defects
- kidney and urinary tract issues
- skeletal abnormalities
- gastrointestinal disorders
- respiratory challenges
- intellectual disabilities
There are three known types of Trisomy 18:
- Full trisomy 18 is when every cell in the body contains an extra chromosome 18. This is the most common and typically the most medically complex form.
- Mosaic trisomy 18 is when only some of the body’s cells carry the extra chromosome. Symptoms may be milder and survival longer, depending on the distribution of affected cells.
- Partial trisomy 18 occurs when a portion of chromosome 18 is attached to another chromosome. This rare type can sometimes be inherited and presents with a wide range of outcomes.
Prognosis and Survival
Trisomy 18 is a condition associated with high rates of miscarriage and infant mortality. For those born alive:
- 60%–75% survive the first week.
- 20%–40% survive the first month.
- About 5%–10% live beyond their first birthday.
While historically survival rates have been very low, advances in medical care and greater recognition of treatment options have led to more children living into childhood, adolescence, and even adulthood. Each child’s journey is unique. Outcomes are shaped by the type of Trisomy 18, the severity of medical complications, and access to timely, coordinated, and compassionate care.
Diagnosis and Inheritance
Prenatal diagnosis is possible through procedures such as amniocentesis or chorionic villus sampling (CVS), which can detect an extra chromosome 18. Full and Mosaic trisomy 18 usually occur as random events caused by errors during egg or sperm formation (nondisjunction). Partial trisomy 18 may be inherited. In these cases, a parent may carry a balanced translocation involving chromosome 18 without showing any symptoms.
Community Conversations
Understanding Trisomy 18: A Spotlight on Community Conversations is a compilation of videos highlighting the personal stories and advocacy journeys of parents, caregivers, clinicians, and individuals living with Trisomy 18. This resource amplifies lived experiences, offering education, hope, and a platform for advocacy.
*🎥 Some videos are provided courtesy of E.WE Foundation partner organizations.
Source: U.S. National Library of Medicine. Medline Plus. http://www.medlineplus.gov | Centers for Disease Control and Prevention. http://www.cdc.gov | Cleveland Clinic. http://www.my.clevelandclinic.org
